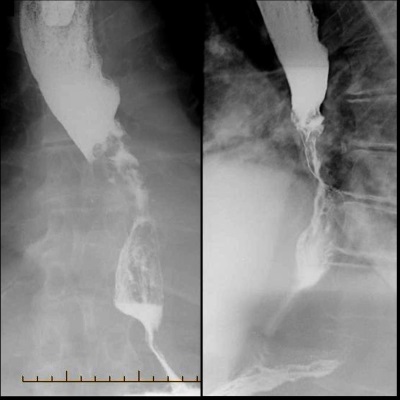
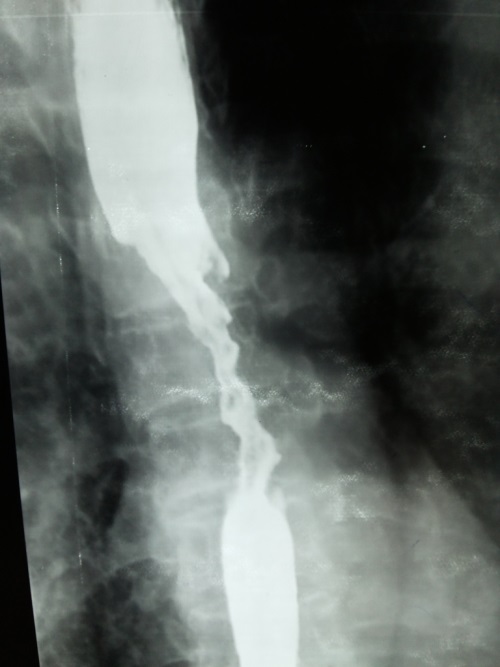
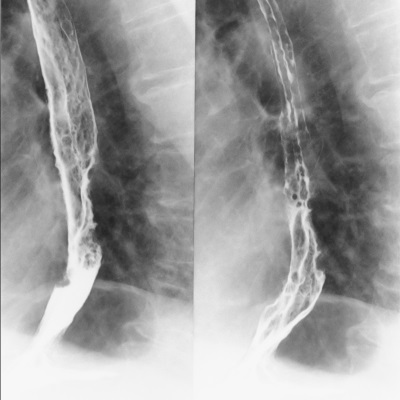
Oesophageal cancer
Until recent times oesophageal cancer was most commonly due to a squamous cell carcinoma but the incidence of adenocarcinoma is rising rapidly. Adenocarcinoma is now the most common type of oesophageal cancer and is more likely to develop in patients with a history of gastro-oesophageal reflux disease (GORD) or Barrett's.
The majority of adenocarcinomas are located near the gastroesophageal junction whereas squamous cell tumours are most commonly found in the upper two-thirds of the oesophagus.
|
Adenocarcinoma |
Squamous cell cancer |
| Epidemiology |
Most common type in the UK/US |
Most common type in the developing world |
| Location |
Lower third - near the gastroesophageal junction |
Upper two-thirds of the oesophagus |
| Risk factors |
• GORD |
|
| • Barrett's oesophagus |
|
|
| • smoking |
|
|
| • obesity |
• smoking |
|
| • alcohol |
|
|
| • achalasia |
|
|
| • Plummer-Vinson syndrome |
|
|
| • diets rich in nitrosamines |
|
|
Features
- dysphagia: the most common presenting symptom
- anorexia and weight loss
- vomiting
- other possible features include:
- odynophagia
- hoarseness: advanced oesophageal tumours, especially in the upper third, may invade or compress the recurrent laryngeal nerve
- melaena
- Tylosis
- diffuse, bilateral hyperkeratosis of the palms and soles - thickened, yellowish plaques that may be painful and fissured
- Although it is non-malignant itself, it has a strong association with oesophageal squamous cell carcinoma (OSCC)
- most commonly inherited in an autosomal dominant pattern with high penetrance. Mutations in the RHBDF2 gene on chromosome 17q25 have been implicated, which affect epidermal growth factor receptor (EGFR) signalling pathways.
Diagnosis
- Upper GI endoscopy with biopsy is used for diagnosis
- Endoscopic ultrasound is the preferred method for locoregional staging
- CT scanning of the chest, abdomen and pelvis is used for initial staging
- FDG-PET CT may be used for detecting occult metastases if metastases are not seen on the initial staging CT scans.
- Laparoscopy is sometimes performed to detect occult peritoneal disease
Treatment
- Operable disease (T1N0M0) is best managed by surgical resection - the most common procedure is an Ivor-Lewis type oesophagectomy
- The biggest surgical challenge is that of anastomotic leak, with an intrathoracic anastomosis resulting in mediastinitis